Feb. 13, 2013 — Dr. Molly Droge is the chair of the subcommittee on access to care at the American Academy of Pediatrics. Growing up in West Texas, she lived next door to an old general practice doctor. She didn’t know him well, but, as she told Remapping Debate, “I did know his reputation in the town, and I knew what his patients thought of him.” He was known for doing everything he could to help his patients, and would often do it without any payment at all. “He got a bowl of tomatoes in the summer, or he got two chickens for whatever care that he had provided someone,” Dr. Droge said. “There was a trust there. And that’s the way I thought doctors acted.”
When Dr. Droge entered pediatric practice in the early 1980s, she joined a managed care organization in Dallas run by Cigna HealthCare and was surprised at how different it was from what she had imagined medicine to be. She found the managed care organization was “all about maximizing profit.” She had difficulty getting necessary referrals for patients. She was forced to try several different medications on patients before she would be allowed to administer the one she knew to be best from the outset, because the best medication wasn’t part of Cigna HealthCare’s list of approved drugs. “Physicians really had to work to make sure that our patients got the care that they needed. It was not a given,” she said.
Dr. Droge’s story is hardly unique. On the contrary, from interviews with health care experts and doctors, as well as in Remapping Debate’s own research into the history of managed care, it appears that the defining feature of the managed care era is a profound rhetorical and practical shift — politically and among health care advocates, observers, providers, and insurers — away from a focus on quality of care and towards an obsession with cost control.
How did this happen? Health care experts suggested the existence of two powerful forces working in tandem. First was the birth and development of the market-based, for-profit health insurance industry, built on the back of what was once a progressive model for how to maximize quality of care: the prepaid group practice, which was later adapted into “managed care.” Second was the spread of an ideology that subordinated quality concerns to cost control while asserting that both could be achieved — an ideology that held particular sway among the New Democrats of the 1990s.
Tracing these two forces requires starting at the origins of managed care: the prepaid group practices that appeared on the West Coast of the United States as early as 1929.
Origins of managed care
The prepaid group practice originated as an attempt to meet comprehensively the health care needs of specific defined communities. The first such practice, the Ross-Loos Medical Group, was created in 1929 by two doctors to care for employees of the Los Angeles Department of Water and Power. Kaiser Permanente, the most famous of the early prepaid group practices and the one most responsible for bringing the model to national attention, was founded by Henry Kaiser during World War II as a medical program for employees of his shipyards and steel mills. Kaiser opened the plan to the public after the war.
Members of these practices would pay an upfront monthly subscription fee, and in return would have all of their health care needs met. The practices were generally physician-led and multispecialty, with the intent of fostering collaboration among doctors and providing all health services under one roof — a plausible prospect for a relatively small practice in an era before the growth of advanced medical technology and countless specialties and sub-specialties. Physicians in such practices were often paid on salary rather than for services rendered.
According to a paper published by the Tufts Managed Care Institute in 1998, the premiums for prepaid group practices “were as expensive or more expensive than other insurance, but their coverage and benefits were superior, including a major emphasis on preventive care, outpatient care, well-child care services, immunizations, and other services not covered by [others].”
Dr. David Himmelstein, a professor of public health at the City University of New York School of Public Health at Hunter College, a visiting professor at Harvard Medical School, and a co-founder of Physicians for a National Health Program (PNHP), sees these early plans as motivated by the desire to find a new model for providing better care: “The prepaid-group-practice era was characterized by a great deal of altruism and [the] conviction[s] that organized prepaid group practice was a better way to care for people and that you could do more for them.”
Dr. Ida Hellander, the director of policy and programs at PNHP, agrees. Cost control “was not the primary motivation,” she said. “The primary motivation was to find a better way of practicing medicine.”
Dr. Georges Benjamin, executive director of the American Public Health Association, added, “It was very much about care over cost.” And Dr. Marc Bard, co-director and physician leader at the Tufts Health Care Institute, said prepaid group practices were “deeply committed to an egalitarian model…The whole idea was that the care provided should be based on the care needed, not on anything else.”
Dr. Jim Scott, president-elect and vice president of internal affairs at the National Physicians Alliance, a multi-specialty medical trade association, noted the practices were seen as radically progressive, but they proved a remarkable success. “They were vilified as socialist or communist organizations, but in fact they delivered demonstrably superior care at a higher value. In other words, good care at a reasonable cost.”
Despite their reputation as radical outfits and their consequent demonization by the American Medical Association and others, the success of the prepaid group practices ultimately caught the eye of some who felt that, with a little tweaking, they could become the key to a revolution in American medicine. Chief among them was Paul Ellwood, a pediatric neurologist who was discontented with the American medical system.
Managed care as public policy: the theoretical origins
In 1970, the Nixon Administration asked Paul Ellwood to consult on an effort to develop a health care reform proposal. Ellwood had been formulating a model of reform inspired by the success of the early prepaid group practices. He is widely credited as the coiner of the phrase “Health Maintenance Organization,” or HMO, to describe the types of organizations pioneered by Henry Kaiser and his contemporaries.
Though Ellwood had been developing his ideas for years, they were most clearly expressed to the public in a 1971 article titled “Health Maintenance Strategy” in the journal Medical Care. In it, he described his proposal for a national strategy to create incentives for the creation and growth of HMOs with federal funds and eliminating any legal barriers to their proliferation.
Ellwood positioned his strategy as a response to the lack of regulation in the American health care system. “Since payment is based upon the number of physician contacts and hospital days used,” he wrote in the article, “the greater the number of contacts and days, the greater the reward to the provider. The consumer, unable to judge his own treatment needs, pays for whatever he is told he needs.” To Ellwood, this lack of regulation meant health care provision “works against the consumer’s interest” and that though care is generally good, “no matter how hard each provider works, services are not available to everyone who needs them.”
Ellwood believed effective government regulation of the health care system was not an option: “Regulation of such scope and complexity would be difficult even in industries which produce easily identifiable goods. It is virtually impossible to do so in a service industry in which professional judgment is required on the level of individual nurses or doctors dealing with individual patients.” The only choice, as he saw it, was to force the industry to self-regulate, and the only way to achieve that was to create a system of competitive market mechanisms in which HMOs, which he felt were “capable of producing services more economically and effectively than conventional providers by integrating and coordinating the many elements of health care,” would compete with one another over cost and quality.
David Himmelstein said the HMO strategy was from the outset intended to create a for-profit health insurance industry dominated by large conglomerates. “The strategy can only be participated in by an organization that includes a large number of primary care doctors, a large number of specialists, and a hospital offering a full range of services,” he said. He estimated that such an organization requires a population base of at least 300,000 to 400,000 people. “Half of the country lives in regions without the population density to support more than one such organization. So what [Ellwood] was really saying was, we’re going to have health care delivered by very large-scale organizations and managed like a business.”
Indeed, Ellwood hoped his strategy would create a free market health care economy which “could stimulate a course of change in the health industry that would have some of the classical aspects of the Industrial Revolution — conversion to larger units of production, technological innovation, division of labor, substitution of capital for labor, vigorous competition, and profitability as the mandatory condition of survival.”
Himmelstein believes the Ellwood article was a major turning point in transforming the American health care field from a not-for-profit system into a for-profit industry. Ellwood, he said, was the first person to make the argument that the provision of health insurance, and hence the provision of health care could have the characteristics of industrial production. “Before that there were really professional incentives — ‘we can do better, organizing ourselves in a better way.’” Ellwood’s argument laid the theoretical groundwork for corporate interests to begin a relentless scramble for profit, but it took an act of public policy to fully open the door.
Managed care as public policy: the political origins
According to Theodore Marmor, a professor emeritus of both political science and public policy and management at the Yale School of Management and the co-author of “Politics, Health, and Health Care,” Ellwood’s ideas caught the eye of a group of what Marmor called “liberal Republicans from California” in the Nixon Administration. They included Robert Finch, the secretary of Health, Education and Welfare (HEW) and later a private counselor to the president, and Lewis Butler, an assistant secretary at HEW. They encouraged President Nixon to use Ellwood’s ideas as the model for a reform proposal, and on February 18, 1971, Nixon announced a new national health strategy centered on HMOs.
Nixon’s motives for embracing Ellwood’s strategy are not entirely clear. Marmor believes he was looking for “a model of cost containment” in response to the increased rate of health care inflation, which at that point was just beginning to outpace the overall rate of inflation. Himmelstein suspects it was in part a defensive measure designed to neutralize the threat to business interests posed by Senator Ted Kennedy’s single-payer national health insurance bill. (See box titled, “Democrats fight for single payer.”)
“They had to respond with something,” Himmelstein said, “and there was a rising tide of calls for something that would negatively affect the corporate interest in health care,” by which Himmelstein meant a national health program. As evidence, Himmelstein pointed to President Nixon’s announcement of his adoption of the HMO strategy. In that statement, Nixon said, “The purpose of this program is simply this: I want America to have the finest health care in the world — and I want every American to be able to have that care when he needs it.” This adoption of the language of universal coverage, Himmelstein said, was “a direct response to Kennedy. And that’s pretty clearly what was the motivation for Nixon, at that moment, to jump in with that initiative.”
Nixon’s true motives, however, might best be revealed by his infamous White House tapes. A recording from February 17, 1971 captured a conversation between President Nixon and John Ehrlichman, the president’s chief domestic advisor. On the tape, which has been transcribed by the Presidential Recordings Program at the University of Virginia, Ehrlichman brought up the idea of incentivizing the creation of HMOs as a model for reform. Nixon was initially hesitant (“You know I’m not too keen on any of these damn medical programs”), but Ehrlichman argued, “This is a private enterprise one…Edgar Kaiser is running his Permanente deal for profit, and the reason that he can do it… All the incentives are toward less medical care, because the less care they give them, the more money they make.” Nixon’s response: “Well, that appeals to me…Not bad.” He announced his HMO plan the next day.
Over the next two years, Congress developed a bill based on Ellwood’s model of reform. The final legislation, the HMO Act of 1973, was a compromise between the bill that emerged from the House of Representatives, which was sponsored by Congressman Paul Rogers and aligned fairly closely with President Nixon’s proposal, and the Senate version of the bill, sponsored by Senator Ted Kennedy. Both men were Democrats.
The Health Maintenance Organization Act of 1973
The HMO Act of 1973 appropriated $375 million (more than $1.9 billion in today’s dollars) in grants and contracts to federally qualified HMOs for a five-year period, established guidelines for what constituted a federally qualified HMO, superseded “restrictive” state laws that “impede[d] the development of HMOs,” required employers of 25 or more workers who received health insurance benefits to give their employees an HMO option if there was an HMO in the area (the “dual choice” requirement), and empowered the secretary of HEW to regulate HMOs receiving financial assistance under the act. In other words, it offered federal money (and the prospect of new enrollees) to HMOs that were willing to abide by a relatively strict set of rules (HMOs not getting federal funding could ignore the rules).
In addition, the bill included provisions added by Senator Kennedy that were intended to ensure that HMOs would be a vehicle for maximizing the quality of health care and providing it to those who were currently uninsured.
These provisions included an open-enrollment rule that required federally qualified HMOs to accept any person who applied, regardless of medical history, and a community-rating rule that required HMOs to charge all subscribers the same premium, regardless of their history of using services.
Dr. Philip Caper, a member of Senator Kennedy’s staff, told The New York Times in 1975 that the motivation behind Kennedy’s additions was to “get away from the antisocial practices in health insurance…The private sector has not assumed their social responsibility. They are in it to make money. The government should get involved to do what private industry has not done.” That is, provide the highest possible quality care at an affordable price.
According to Theodore Marmor, “The HMO Act of 1973 set in motion the developments that emerged in the ’90s” — referring to the for-profit, conglomerate model that came to dominate U.S. health care in that period.
Loosened restrictions
In attempting to balance the ideology of cost-control and market competition (promoted by President Nixon and other Republicans), with that of maximizing health care quality and access (promoted by Sen. Kennedy and his allies), the final bill that emerged was unable to fully realize either set of goals. Both parties were unsatisfied, but the GOP’s initial view came to have more and more sway. Over the next two decades, a series of amendments loosened the restrictions of the bill, effectively gutting the Kennedy provisions. These amendments were signed into law by President Ford in 1976 and by President Reagan in 1988. (They stripped, among other things, the requirement that federally qualified HMOs cover “supplemental benefits,” including long-term care facilities, vision, dental, drugs, and rehabilitative services.) In addition, President Carter signed a bill in 1978 extending grant funding for HMOs, as the original five-year allotment was set to expire.
The burgeoning for-profit health insurance industry was, unsurprisingly, the loudest voice in favor of amending the HMO Act. A large group of health insurers created a lobbying outfit called the Consensus Group, which argued the law was too stringent to allow federally qualified HMOs to compete with those who chose to simply bypass the federal seal of approval (and the grants that went with it). To them, the HMO Act “require[d] HMOs to be better, more humane and more generous than the entire health and delivery system of which they are a part” (criticizing, in other words, the precise point of Senator Kennedy’s additions to the bill).
Over the course of the 1970s and 1980s, the federal government continued to actively promote HMOs as a cost-saving mechanism. The most notable example of this effort came from the Carter Administration. Secretary Joseph A. Califano Jr., President Carter’s secretary of HEW, held a marketing blitz to encourage the private sector to invest in HMOs. He held a conference on May 10, 1978, in which HEW staff, health insurance insiders, and pro-HMO business leaders addressed representatives of more than 600 corporations on why they should move toward HMOs as the primary mode of providing health care to their employees. An article in The Washington Post described Califano’s goal as being “to help reduce health care costs by supporting potentially money-saving health maintenance organizations.” According to the article, Paul Parker, the executive vice president of General Mills at the time, told the conference how the HMO his company sponsored “reduced health care costs by drastically cutting hospitalization.”
Managed care begins to catch on
Due in part to the efforts of the federal government, HMO enrollment steadily climbed throughout this period, though HMO enrollees remained overall a small portion of the American population. In 1970, 3 million Americans were enrolled in HMOs; that number climbed to 10 million in 1980 and to 32 million in 1990. The business model of HMOs was changing, too. According to data from the Kaiser Family Foundation, 88 percent of HMOs were not-for-profits in 1981. By 1993, only 48 percent of HMOs were not-for-profits.
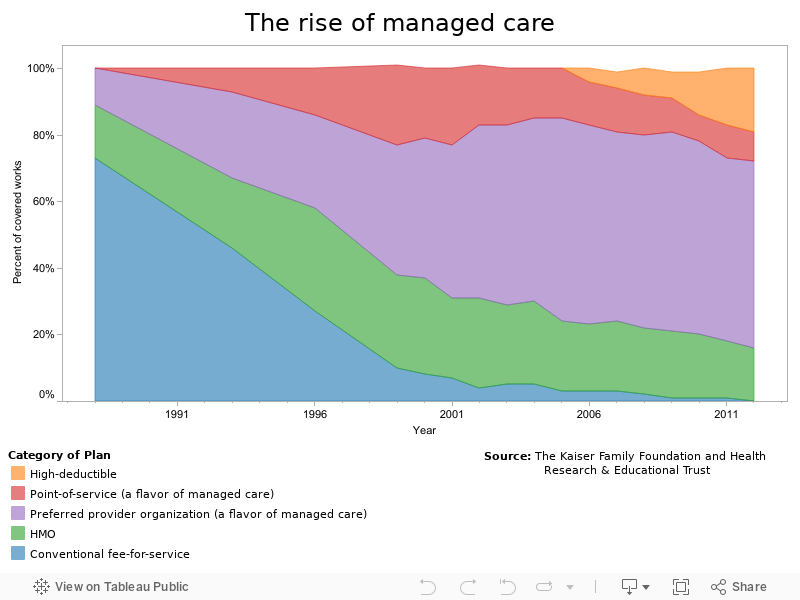
The overall health insurance industry, however, was still dominated by traditional fee-for-service insurers. In 1988, the earliest year that such data is available, 73 percent of American workers with health insurance had a traditional fee-for-service plan, with the remaining 27 percent in some form of managed care.
Those figures were soon to reverse at an astonishing speed — a process that was driven by the proliferation of other forms of managed care, most notably Preferred Provider Organizations (PPOs) and Point of Service (POS) plans.
These were variations on the basic principles of HMOs: capitation (in which physicians are paid a set amount for each patient per period of time, regardless of the services rendered), gatekeeper physicians (a primary care physician assigned to a patient who must approve all referrals to specialists for those services to be covered by insurance), and networked doctors (doctors who contract with the same insurance plan; depending on the type of managed care plan, doctors outside that network might be more expensive for patients, or might not be covered by insurance at all). They offered some greater flexibility than the “pure” HMOs that had sprouted in the 1970s and 1980s, but retained the underlying principle: to control cost and make a profit.
The managed care explosion of the 1990s
By 1993, managed care had become the primary form of health coverage in America. 46 percent of workers had a fee-for-service plan, with 54 percent in managed care. In 1996, only 27 percent were left in fee-for-service; in 1999, only 10 percent.
What caused the enrollment explosion? According to Dr. Himmelstein, one major factor in this was the concern among corporations that health care costs were growing too quickly. “There was a perception and a reality that costs were an issue,” he said. “They were an issue for the first time for corporate purchasers of care. It wasn’t just out-of-pocket costs that were going up, but you had the auto industry for instance beginning to say, ‘We can’t afford these [rising health insurance costs].’ In the ’90s that was certainly a major push.”
Dr. Jim Scott agreed: “If you’re an employer, it wasn’t such a big deal when it was a fairly small increase [as it was throughout the 1970s], but then it compounded over the years. That’s why by the late ’80s and early ’90s, [employers] were going ‘Whoa, we can’t afford this continued rate of inflation.’” (See box titled, “The root of rising health care costs.”)
While noting the reality of rising health care costs, Himmelstein said the important question is “how you respond to those cost pressures.” Many employers saw managed care as the solution, and were undoubtedly helped to this belief by the efforts of the federal government over the previous two decades.
Himmelstein contends that corporate interests — and their allies in government — were not merely responding to cost pressure, but exploited the trend toward cost concerns as an opportunity for an “offensive measure.” They used the rising cost pressures of health care as a “crowbar,” he said, in order to advance their own agenda: the transformation of health insurance into a for-profit industry, with the spread of managed care plans as the primary instrument. In the 1990s, they found a partner in the New Democrats.
Coming next week: the New Democrats, proselytizing in favor of market solutions, subordinate concerns about quality of care to an all-consuming desire to control costs and ignore what some say was a patently obvious conflict between the interests of for-profit insurers and those of the patients that the insurers were being relied on to serve.
This article has been edited (March 5, 2013) to make clear that Paul Ellwood was working with the Nixon administration to formulate an HMO-based strategy for health care reform even prior to his 1971 “Health Maintenance Strategy” article.